Case Studies in COVID-19 Defensive Record-Keeping

COVID-19 has brought new risk for claims against LTC facilities. Since inception of the COVID-19 pandemic, some insurers have already seen hundreds of individual COVID-19 claims. With senior living facilities accounting for 35-40% of COVID-19 related deaths, it is critical that long-term care (LTC) facilities properly train staff and mitigate risk through preventive measures such as tracking and maintaining information and defensive record-keeping. Learn why defensive record-keeping is important through these case studies.
What is defensive record-keeping?
Defensive record-keeping is maintaining proper and complete records to support the level of care given in facilities. These comprehensive records can be used to fight litigation claims. Without defensive and thorough record-keeping, organizations expose themselves to unnecessary risk. Failing to implement proactive defensive record-keeping strategies makes LTC facilities particularly prone to risk during COVID-19.
“Defensive record-keeping is maintaining proper and complete records to support the level of care given in facilities.”
Not only does a lack of proactive systems make LTC facilities vulnerable to unnecessary and costly litigation but can also affect the standard of care facts in a case, should litigation support be needed. For example, a lack of defensive record-keeping may result in an inability to support prompt detection, triage, and isolation of potentially infectious residents. The adage here stands true: if it wasn’t documented, it wasn’t done. It becomes more critical with an outbreak in senior-living facilities to record resident data properly.
How to implement defensive record-keeping
One of the best ways to mitigate future risk is through enhanced staff training in defensive record-keeping. Given the profound impact COVID-19 is having in the senior-care environment and the volatile nature of litigation in this area, it’s more important than ever that staff understand the importance of memorializing resident assessments and the overall care being rendered in the medical records. Healthcare organizations must have a strategic and consistent approach to record-keeping to ensure all staff are properly recording data and resident information.
Strong record-keeping equals a strong defense in medical-legal matters. Accurate and clear documentation in the medical record supports the staff’s prompt and appropriate actions to reduce transmission and minimize the impact of COVID-19. The following case studies clearly outline the need for proper and proactive mitigation and defensive record-keeping.
Case Study 1: Failure to Adequately Document Basic Clinical Assessments
Long-term care residents are at an increased risk for contracting COVID-19 and having significantly worse outcomes secondary to age and the presence of comorbid conditions typical in the aging population. Basic screening measures, such as timely and comprehensive physical examinations, are the foundation of clinical practice and enable nurses to systematically assess residents and prioritize care. Actively monitoring for symptoms of COVID-19 is essential due to the rapid decline noted in many patients presenting with the disease. Staff should be diligent in their efforts to regularly record physiological observations and seek out additional clinical signs and symptoms, observing trends outside the resident’s baseline.
The following chart examples demonstrate a failure by the staff to thoroughly document the resident’s respiratory status and details of respiratory changes noted as a part of the clinical assessment performed.
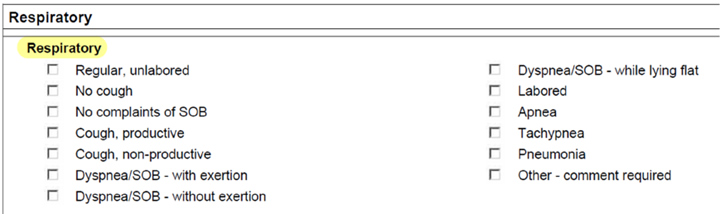
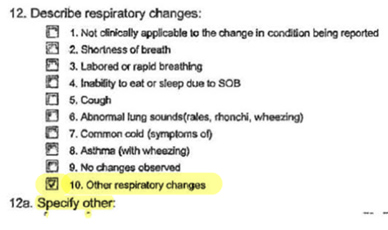
The staff’s failure to ensure accurate and clear documentation in the medical record undermines their efforts put forth to provide comprehensive, patient-centered care and increases the litigation risk posed by documentation holes in the medical record.
Case Study 2: Inadequate Oxygen Saturation Documentation
Underlying health conditions and the advanced age of many long-term care residents places these persons at risk for severe morbidity and death. Staff should consider the evaluation of risk levels for all residents and the implementation of heightened screening measures for those at greatest risk. This may include increased frequency of monitoring of respiratory status (symptoms of cough, nasal discharge, shortness of breath) and O2 saturation levels, vital signs, pain, and mental status. Staff should ensure clinical assessments are consistent, and documentation thoroughly supports the careful care being rendered. This is exceedingly important for those residents with an already compromised respiratory or immune status or those requiring oxygen therapy.
The following chart examples demonstrate incomplete documentation of oxygen saturation levels in residents receiving O2 therapy.
7 out of 12 oxygen saturation assessments omitted:

Lack of documentation of O2 saturations for 6 shifts:
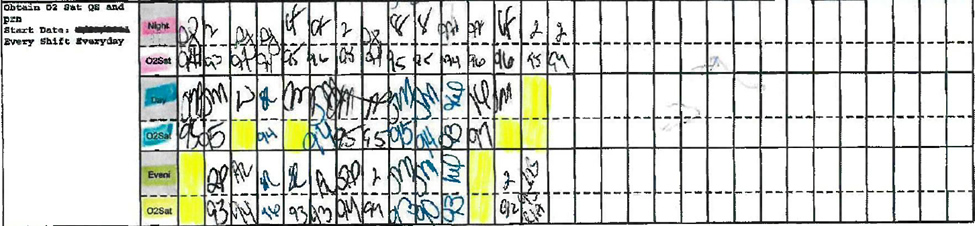
The staff’s failure to properly substantiate the residents’ monitoring under their care unnecessarily increases the facility’s risk for litigation. The facility staff should be cognizant of the need to provide comprehensive, patient-centered care, and the claims risk posed by inadequate documentation.
How Med Law Advisory Partners can help
Med Law Advisory Partners can help LTC organizations implement action plans to help mitigate risk for claims associated with COVID-19. Our COVID-19 Liability Defense Preparedness Program can help LTC facilities manage risk and effectively respond to these claims. Through an in-depth audit, our team of legal nurse consultants identifies weaknesses in record-keeping systems and outlines ways to improve processes. Then, we help define and put in to practice a strategic record-keeping protocol for staff. In the event of litigation, our legal nurse consultants can perform extensive medical record reviews to help defend standard of care claims.
Some insurers have already seen hundreds of individual COVID-19 claims since the pandemic began. Now more than ever, it is important to identify charting pitfalls and implement action plans to empower staff to maintain comprehensive records. LTC facilities in particular must be proactive in managing the risk of litigation through defensive record-keeping during and beyond the COVID-19 pandemic. As we have seen in our case studies, the pitfalls of improper record-keeping expose organizations to unnecessary risk and threaten an organization’s ability to defend against litigation.
If you would like more information on how your organization can proactively mitigate risk of COVID-19 claims, we’d like to hear from you.
 Founded by Alicia Davis, RN, LNCC, Med Law Advisory Partners (and former ALN Consulting) provides resources and expertise in the areas of safe opioid prescribing, medical malpractice and post-acute care litigation, including COVID-19 claims. Alicia and her team have worked with government entities, healthcare systems, insurers and senior-living operators for nearly 20 years, helping mitigate risk and manage medical-legal and healthcare fraud claims.
Founded by Alicia Davis, RN, LNCC, Med Law Advisory Partners (and former ALN Consulting) provides resources and expertise in the areas of safe opioid prescribing, medical malpractice and post-acute care litigation, including COVID-19 claims. Alicia and her team have worked with government entities, healthcare systems, insurers and senior-living operators for nearly 20 years, helping mitigate risk and manage medical-legal and healthcare fraud claims.